“What Are the Uses of Disability Models? A Neo-institutional Response: Traditions, Rupture, and Power1 “
Pedro Nuno de Oliveira*2
* Independent Researcher, Instituto Português de Relações Internacionais da Universidade Nova de Lisboa
Abstract: Given the persistent intergenerational experiences of exclusion, prejudice, institutional care, and welfare approaches towards disability, this article argues that there are more continuities than ruptures between disability models that have established societal responses to the needs of disabled people. The article analyses how these models effectively differ from each other in terms of their responses to the needs of disabled people, drawing on neo-institutionalism and the historical construction of disability, disability models, and historical traditions.
Keywords: neo-institutionalism, historical construction of disability, disability models, historical traditions.
Introduction
The status of institutional studies in political science has changed dramatically in recent years, with a neo-institutionalist resurgence in political science (March & Olsen, 2006; Pierson & Skocpol, 2002).Political institutions are not only reflective of history and political thought, but also of culture, arenas of conflict, architecture, rules, and processes that ensure the regular functioning of societies, determine opportunities and incentives for behaviour adoption, inclusion and exclusion of potential actors, the relative ease or difficulty of inducing change, and the mechanisms through which the production of new institutional logics can be realized or thwarted (Rhodes et al., 2006; von Beyme, 2006).
Using a neo-institutionalist perspective, the central argument of this article is that despite an axiological rupture3 concerning parameters of Western societal thinking about disability, supposedly materialized in the shift between disability models4, this reality has been unable to break with thetradition of creating segregative solutions to meet the needs of disabled people. Consequently, therehas been a persistent continuity of exclusionary, prejudiced, segregationist, and welfare-oriented patterns in the life experiences of these individuals from generation to generation.
This leads us to posit that there are more continuities than ruptures between the disability models.Furthermore, this notion appears to support the idea that invariance is a characteristic of traditions(Hobsbawm & Ranger, 1983), conceptualized in this study as political institutions. It reinforces the perspective that political institutions can be perceived as enduring phenomena (Pierson, 2005, 2006).
Thus, to confirm or question the usefulness of using these models in the institutional study of disability, this study focuses on answering two questions:
1. Is there variation among disability models in terms of attitudes and responses to the challenges and issues inherent in this social reality?
2. How has variation among disability models influenced the power dynamics of different actors involved and impacted the development and trajectories of political institutions?
Therefore, in the subsequent sections, I will delve into an initial era extending from Antiquity to the 14th century, during which mystical, religious, and moral thought played a pivotal role in shaping social order and practices. The second period, commencing with the emergence of Renaissance thought in the 14th century and extending until 1930, witnessed the rise of scientific and medical perspectives, accompanied by the professionalization of the disability field. The last period, spanning from 1930 to the present, has been predominantly influenced by the doctrine of human rights, giving rise to family, community, and consumer models. In the conclusion, I will undertake a comprehensive cross-sectional analysis to address the initial questions.
1 Moral Model of Disability
One of the first observations that arises when studying Antiquity is that disabilities, incapacities, and deformities were a predominant reality due to the omnipresence of diseases, wars, poor prenatal care, malnutrition, and injuries suffered in workplace accidents. Even small injuries such as broken limbs produced disabling disabilities in most of the population, who were too poor to obtain medical care (Garland, 1995).
The exposure of disabled children in Ancient Greece was limited to deformities considered aberrations in relation to the human species (Stiker, 1997), excluding congenital or acquired sensory impairments. This practice was motivated by economic factors, driven by the extreme poverty of families, as well as religious reasons attributing their birth to divine anger, wherein exposing them was viewed as an act of returning to the divine. Additionally, exposure occurred for community reasons, as these births were seen as announcements, foreshadowing, and symbols of divine condemnation at the social and moral levels. Consequently, disability evolved into a societal and political issue (Stiker, 1997).
However, Garland (1995) argues that this practice was not as widespread as commonly believed, aligning with Stiker’s conclusion (1997) that the presence of adults with congenital disabilities in Ancient Greek society was a reality. Finally, it is crucial to note that the family-based mode of production, characteristic of this agrarian society, did not exclude disabled people from active participation in their local communities (Finkelstein, 1980; Lang, 2001).
The reviews by Edwards (1996, 1997) and Parish & Braddock (2001) on the historical records of ancient Greece provide other relevant observations beyond the phenomenon of child exposure. During this period, acquired disabilities were perceived as a normal aspect of the course of life5 people with developmental disabilities or mental illness were kept at home to prevent situations of misconduct, although madness would be seen as a positive manifestation of the divine. Deaf and mute people were seen as inferior while blind people were considered “normal” and enjoyed their full rights (Stiker, 1997). It could be argued that today, compared to the past, developmental disabilities or mental illnesses have descended in the hierarchy of social acceptance, falling to the level of more stigmatized disabilities (Clapton & Fitzgerald, 1997). The findings of these investigations also indicate that there is no evidence to suggest that individuals with disabilities during this period self-identified or were identified as a minority group (Edwards, 1997).
In ancient times, only diseases were seemingly associated with sinful acts, injustice, adultery, incest, and pollution, which warranted rejection by the human community. But during this period, “psychomoral medicine” and the belief that individuals with disabilities possessed a supernatural nature or were influenced by supernatural forces (Colón, 1989), 1989) coexisted with more rational, technical, and clinical modes of thought associated with Hippocrates. In the mental universe of the Egyptian civilization, disabilities lost their pathogenic essence and became viewed as something shamanic, which could be purged through rituals and charms.
Regarding the relationship between disability and access to power, it can be said that since disability was viewed as a normal aspect of life and the community living of disabled people was common and significant, it is expected that many kings and emperors may have acquired disabilities themselves.
It is important to say that myths in antiquity such as those of Oedipus, Philoctetes, and Hephaestus are good examples of how mythology used deformity, disability, and incapacity as symbols of societal characteristics (Delcourt, 1986; Girard, 1972, 2001).
From Jewish society to the Christian era, sacred texts also mention disabilities, suggesting that it was a daily reality during this period with socio-religious implications (Leviticus 13: 16-246). Legal impurity was associated with disabled people, the same status attributed to prostitutes or menstruating women. This meant that these people could participate in various worship rituals, except for sacrifices to maintain the purity of the sanctuary. This prevented the participation of these people in the priestly function, which was essentially understood as mediation between God and the people. Disabled people were also excluded from communal meals and exempt from military service to ensure the holiness of the congregation.
Regarding the Old Testament biblical text, I could say, almost paradoxically, that within the coherence of the ancient Jewish system, the non-integration of disabled people in religious practice was a necessary condition for their non-societal exclusion, even if in certain very specific cases, due to fear and prophylaxis, there was an aspect of social rejection.
The New Testament decisively breaks with the connotation between disability and individual guilt without ending the religious prohibition that affects disabled people. But by explicitly saying that the sick, disabled people, and marginalized people are the first in the Kingdom of God and by reaching out to those who were subject to the law of prohibition, or by letting them come to Him, these acts of Jesus have an extremely destabilizing character at the level of the social system and introduce, at the same time, a problem that is extremely difficult to assume: our relationship with disability and “abnormality” becomes an entirely personal issue.
Finally, and despite recommendations for the home isolation of people with mental disorders as a preventive measure to maintain public order, and sanitary care for lepers that led to their segregation in leprosariums, the community living of disabled people was also a reality in biblical societies. This leads us to assume that the main support for these people was their families and their communities, and not any institutional system of care (Stiker, 1997).
The Middle Ages witnessed a significant shift in the dynamics between society and individuals with disabilities. This era saw a diversification and intensification of prejudices that fuelled the persecution of disabled individuals. Additionally, segregation institutions began to emerge from the 4th century AD. Notably, asylums catering to individuals with mental disabilities were established by the Arabs in the eighth century. Unlike prevailing beliefs in some other cultures, the Arabs generally considered mental disability to be divinely inspired rather than demonic. Consequently, the care provided in these facilities was characterized by a benevolent approach (Parish & Braddock, 2001; Winzer, 1993).
On the other hand, the absence of references to demonology, a recurrent justification for explaining the difference in medical texts of the time by advocates of natural causes of mental illness, proves the existence of alternative attitudes towards these people in the Late Middle Ages (Parish & Braddock, 2001; Stiker, 1997; Winzer, 1993).
The relationship between poverty and disability during the medieval period is also significant. In the 13th century, tax records from France, Italy, and England indicate that 75% of the population was too poor to pay taxes and was particularly vulnerable to disease and disabilities due to malnutrition, making these people quite visible in their communities (Farmer, 1998; Jankauskas & Urbanavicius, 1998). Primarily due to their poverty, these people survived depending on the support of family members, neighbours, employers, and begging (Farmer, 1998). Charitable institutions seem to have been the least likely source of support for disabled people. Given their high number, the existence of the poor was accepted as part of the natural order and as an opportunity for wealthier citizens to do good by giving them alms. Guilds and brotherhoods of blind beggars were also organized (Covey, 1998; Farmer, 1998; Parish & Braddock, 2001).
2 The Medical Model of Disah2ility
This period is marked by the gradual emergence of scientific thought and professional elites in a context of transition between agrarian, mercantilist, and industrial societies. It is during this period that disability becomes an individualized, and medicalized phenomenon (Barnes & Oliver, 1993; Finkelstein, 1980; Lang, 2001; Parish & Braddock, 2001).
Despite the progress in human knowledge during the Renaissance, the belief that disabled people had a supernatural nature or were influenced by supernatural forces continued during the early modern period (Colón, 1989; Parish & Braddock, 2001). In England, at the beginning of this period, society conceived two groups of people with developmental disabilities or mental illnesses: the “safe” and the “dangerous,” with many people belonging to the first group (Parish & Braddock, 2001; Rushton, 1988; Suzuki, 1991). These individuals were generally under the care of their families, who had unclear but diversified support from their local communities (Andrews, 1998; Rushton, 1988).
From the 12th century, the notion that poverty was a divine blessing, and beggars represented an opportunity for benefactors to please God, slowly transformed into the belief that poor individuals were dangerous. By the 16th century, this shift in attitudes was complete, leading to the establishment of incarceration facilities for mentally ill people (Parish & Braddock, 2001). Another significant development during the 16th century was the initiation of education for the deaf. Initially, the first deaf children to receive education belonged to aristocratic families and were concealed in Spanish monasteries and convents by their affluent relatives (Plann, 1997). Although deaf education remained confined to the upper classes in the subsequent century, it began extending beyond monasteries (Daniels, 1997; Miles, 2000; Parish & Braddock, 2001). Consequently, between the 16th and 18th centuries, there was also a gradual proliferation of residential schools for deaf and blind individuals.
England’s Poor Law of 1601 defined specific family and community responsibilities for the poor and other unable to support themselves for the first time (Axinn & Levin, 1982; Rushton, 1988, 1996). As a result of this legal framework, most disabled people remained in the community with their families, except for mentally ill people who were incarcerated in prisons and correctional homes (Adair et al., 1997; Cavallo, 2013; Rushton, 1996). What is particularly important about the administration of welfare at this time is that it “marked a shift from the predominantly familial system that dominated the medieval period” (Rushton, 1988, p. 34).
During the 18th century in England, the proliferation of reception asylums led to the incarceration of the “furiously insane” without treatment, gradually removing disabled individuals from community spaces. Despite serious inadequacies in these facilities, the British Parliament, while repealing witchcraft acts, demanded improvements in conditions at private asylums (Parish & Braddock, 2001).
Foucault’s perspective (1973) highlights the classical era’s transformation in society’s approach to madness. Specialized structures and distinct control methods aimed to silence madness, stripping the mad individual of articulate thoughts during confinement. This act of confinement not only silenced madness but also subjected it to reclassification as social deviance associated with negative perceptions of labour. The Renaissance views on madness, allowing it to express freely, sharply contrasted with the classical era. Foucault suggests that the diverse and seemingly successful measures used during the classical period were “strange.”
The Classical Age, influenced by the Renaissance intellectual revolution, witnessed the medicalization and professionalization of disability. This era saw the emergence of a professional class, including doctors, educators, and caregivers, fostering institutional care solutions. Segregated schools and workshop schools within European educational institutions became prevalent in the mid-19th century. In 1829, Louis Braille published an improved braille system, refining the one developed by Barbier in 1808 (F. K. Roberts, 1986).
Foucault (1973) notes a transformative shift in the 19th century when confinement was condemned not only as a humanitarian concern but also as an economic mistake. The asylum emerged as the new institution, portraying the madman as a moral outcast. Caregivers aimed to shape the conscience and guilt feelings of the madman. The family model became the new framework for understanding and addressing madness. By the late 19th century, madness wasincreasingly perceived as moral degeneracy, paving the way for a new doctor-patient relationship.
The 19th century also marks the beginning of differential diagnosis, evaluation, and treatment of speech disorders (Rockey, 1980). In Spain, oralism was decreed, and deaf students, based on the belief that they were defective and unintelligent, were encouraged to learn manual trades and subjected to considerable physical abuse. There was also a strong rejection of deaf teachers, and the education of deaf students was left to hearing specialists (Plann, 1997). In 1872, Alexander Graham Bell advocated for the suppression of sign language and opened a school for teachers in Boston with the intention of encouraging deaf people to “pass” as hearing individuals. In 1880, a resolution was passed at the International Congress on the Education of the Deaf that prohibited the use of sign language by these students (Lane, 1989). In direct response to this prohibition, one of the first self-advocacy organizations for disabled people emerged in 1890.
Therefore, it is evident that the implementation of segregation institutions was an ongoing process that commenced in the 4th century AD, solidified by the 18th century, and in the last decades of the 1800s became globalized. This process impacted all groups of disabled individuals with varying intensity, and treatment gave way to the confinement and custodial care of patients who were described as extremely dangerous in large facilities. This situation led to overcrowding and impoverished conditions in these asylums at the end of the 19th century. Rothman (1990) and Scull (1991) argue that those in charge used this situation to demand more equipment, legitimize their own existence, and ensure their power. The growing concern about the number of disabled people in the United States resulted in their enumeration in the censuses, as Parish & Braddock (2001) report. Until 1840, deaf and blind people were initially counted, and later, those labelled “idiots” and “crazy.”7
The crisis reinforced the lifelong custodial role of institutions for disabled people due to extensive unemployment, making it increasingly difficult for these graduates to find employment outside the facilities (Trent, 1995), and resident labour exploitation prevailed in these institutions until the late 1960s (Parish & Braddock, 2001).
At the dawn of the 20th century, in addition to these institutions, the so-called freak shows were another form of exploitation of disabled people that served to reinforce the notion of normalcy by emphasizing disability and raceas deep and monstrous differences (Bogdan, 1988; Rothfels, 1996; Thomson, 1996, 1997). The widely disseminated eugenic belief between 1880 and 1925 was that mental disability was an incurable, hereditary disease that degraded the species (Switzky et al., 1988; Trent, 1995). In numerous studies, this belief was associated with criminality, immoral behaviour, and pauperism (Parish & Braddock, 2001). The combination of the emergence of economic problems and the diffusion of ideas about social Darwinism caused those in charge of institutions to strengthen arguments about the need for institutional care to legitimize and consolidate their authority (Trent, 1995).
The approval of the country’s first universal civil law on vocational rehabilitation in 1920, following the creation of rehabilitation services for soldiers returning from World War I with disabilities, highlighted the great importance of charitable organizations (Parish & Braddock, 2001).
Before concluding this section, it is worth reflecting on the argument that the Industrial Revolution played a significant role in marginalizing disabled people in the West during the modern era. The Industrial Revolution commenced in the second half of the 18th century and brought about significant changes in the world economy, labour relations, and human lifestyle, marking the formation of capitalism (Mokyr, 1998; Stearns, 2012). However, scholars, including materialist, socioconstructivist, and Marxist thinkers, have criticized capitalist industrial development. They argue that industrialization marginalized disabled people due to material barriers limiting access to wage labour. The main contention of these scholars is that, although disabled people may have experienced poverty and stigma in the pre-industrial era, the structure, flexible nature, requirements, and expectations of the agrarian economy and pre-industrial life allowed them to assume productive roles or socially valued positions (Erevelles, 2001; Finkelstein, 1980; Gleeson, 1999; Oliver & Barnes, 2012; Richards, 2009).
Is this a consensual historical fact?
For Blackie (2018) or Turner & Blackie (2018), this argument relies on oversimplified views of the Industrial Revolution that undermine its explanatory power. Taking the British coal industry in the 19th century as an example, they argue that disabled people were frequently present in the industrialization process, as disability and health issues were considered natural and unavoidable consequences of industrial work. The significance of miners to Britain’s economic success and material well-being was widely acknowledged, and those who suffered workplace accidents were seen as deserving of community support and sympathy, much like injured military personnel.
However, these workers often faced greater workplace risks due to their disabilities, and while they participated in production, it was typically in less prestigious or lower-paying roles. Although, if coal mining represents broader economic trends that occurred during British industrialization, this continued involvement of disabled people in the coal mining workforce truly challenges the idea that the Industrial Revolution was a major factor in their marginalization, as suggested by materialist scholars (Berg & Hudson, 1992).
On the other hand, 21st-century sociological studies suggest that injuries resulting from workplace accidents can have a masculinizing effect in some contexts, especially in physically risky occupations. In industries characterized by a hyper-masculine work culture, injuries are often celebrated as signs of masculinity. Miners with disabilities employed on the surface, the “boys’ work,”may have faced a challenge to their masculinity because of their injuries, but those same injuries may also have provided an effective buffer against the worst devastations of emasculation.
That is to say, the experiences of workers with disabilities during the Industrial Revolution were diverse: at the level of the body, different disabilities affected the lives of disabled people in varied ways. The interaction of these disabilities with the work environment also depended on the type of work performed by disabled people (Blackie, 2018). And if we adopt a broader and more accurate concept of the nature of work in industrial societies, which goes beyond the changes associated solely with factory production and mechanization, the Industrial Revolution will seem less disruptive to the work lives of disabled people than is often assumed (Berg & Hudson, 1992; Blackie, 2018; S. F. Rose, 2017; Turner & Blackie, 2018).
Therefore, Ishare the belief of Turner and Blackie (2018) that the argument that economic change, especially industrialization, marginalized disabled people in the workforce should be approached critically and supported by comparative studies that analyse different economic sectors, regions, nations, and periods that help to better understand the consequences of economic change for disabled people.
3 Family, community, and consumer models
During the period that commenced in the 1930s, a coexistence of the hegemony of professional and ecclesiastical elites and alternative and challenging proposals of a family, community, and consumer nature was observed. This hegemony was established through an unequal distribution of power resources such as knowledge, influence, and control over installed social services supply.
From an organizational development perspective, it can be observed that families of individuals with intellectual disabilities in Washington started to organize themselves in the 1930s to advocate for the implementation of services for their children (Grob, 1994; Jones, 1987; Lefley, 1996). In the 1940s, to increase the public awareness of the poor conditions in American psychiatric hospitals and to the need for advanced research in the field of mental illness due to autobiographical reports. Even though the institutionalist orientation remained dominant, this led to the creation of the National Institute of Mental Health and the largest network of community services for people with mental illness in the United States (Braddock, 1986; Parish & Braddock, 2001).
However, it was not until the early 1950s that family and friends of disabled people began to create more comprehensive services. This period of organizational development coincided with the introduction of antipsychotic drugs in the 1950s and a public commitment to a community-based treatment approach, which resulted in a rapid reduction in the institutionalized population (Grob, 1994). However, the overall decline in the population residing in these institutions during this period only tells part of the story, as admissions and discharges from overcrowded psychiatric hospitals functioned as a revolving door for many patients (Grob, 1994; Lefley, 1996).
In the 1960s, many of the recommendations of the presidential panel appointed by Kennedy administration in 1961 were signed into law by Congress, covering various areas such as civil rights, the orientation of innovation in service delivery, substantial reduction of the number of institutional facilities, expansion of community services, and the need for scientific research on etiology and prevention. President Kennedy also signed the 1963 law that created community mental health centres, propelling the development of these centres across the country as part of a community support network (Grob, 1994). The first organizations led by disabled people emerged in the United States appear in this decade, and there were instances of organizations whose leadership shifted from people without disabilities to disabled people (E. Roberts, 1989).
In the transition from industrial societies to the information society towards a global knowledge society, a significant evolution occurred, marked by the consolidation and intricate development of scientific thought. This transformative period was characterized by technological acceleration and the tertiarization of the economy (Innerarity, 2012; Välimaa & Hoffman, 2008). As we delve into the societal landscape of the 1970s, a pivotal era, it becomes evident that this backdrop laid the groundwork for substantial shifts in various domains, including academic, social, and political spheres. This dynamic context sets the stage for the emergence of influential paradigms, such as the social model of disability, which challenged prevailing perspectives on disability and paved the way for a more inclusive and socially conscious understanding.
The social model generated a set of academic publications predominantly written by scholars and activists with disabilities, which is the complete antithesis of the medical model (Davis, 1997; Linton, 1998; Oliver, 1990). Members of the Union of the Physically Impaired Against Segregation (UPIAS) argued that disability was a complex form of social oppression like that faced by women, ethnic and sexual minorities (Parish & Braddock, 2001). Thus, the social model of disability serves as a ‘heuristic device’ that draws attention to the limitations of individual interventions in terms of promoting the empowerment of disabled people. It is a deliberate attempt to highlight the problems caused by environmental and cultural barriers that oppress these individuals, regardless of the political, economic, and religious context of the society in which they live, and which inevitably harm their personality and status as full citizens (Oliver, 1983).
However, the social model of disability should not be viewed as a monolithic entity but rather as a collection of versions and approaches that seek to comprehend the notion of disability. Janine Owens (2015) identifies three versions of the model:
1. The United Kingdom (UK) version, typically associated with materialist, socioconstructivist, and Marxist perspectives;
2. The Nordic version (primarily Swedish), a product of the salutogenic approach to health
and a reflection of the post-industrial welfare model, and;
3. The North American version, which is linked to the disability rights movement.
Critiques of the social model of disability can be categorized into three distinct viewpoints. The first viewpoint concerns the relativization of the body, whereby the UK social model of disability distinguishes illness and disability as separate entities, relinquishing the analysis of the “variable”body to medical interpretation. This neglects the fact that chronic illness or pain may reduce activity and participation to a degree where external restrictions become irrelevant (Crow, 1996; Hughes, 1999; Hughes & Paterson, 1997; Marks, 1999; Oliver, 1996; Shakespeare & Watson, 2001). By defining disabilities and impairments in terms of their consequences, the analyses of this model end up overlooking cognitive, acquired, and fluctuating disabilities because social adaptation is not always feasible. This results in analytical devaluation of personal and social differences and a narrative that emphasizes societal oppression and differences between people with and without disabilities (Corker, 2002; Terzi, 2004; Williams, 1999).
The second viewpoint centres on societal oppression, with disability politics critiquing oppression as the main component of disability. However, oppression is a poorly understood and under-theorized concept, and the social model of disability struggles to fully theorize the experiences of disabled people who live with impairments. It relies on the belief that the practice of solidarity will lead to liberation, which leaves little room for recognizing individuality and undermines the ethos of solidarity (Hughes, 1999; Imrie, 1997; Shakespeare, 1994).
The third viewpoint highlights the inadequate theoretical basis of the social model of disability. There is a need to develop the components of disability further to enhance the explanatory power of the social model (Corker, 1999; Finklestein, 2001; Longmore, 2003).
Apart from these critiques, the interpretative, explanatory, and empirical fragility of radical materialism (Finkelstein, 1980; Gleeson, 1999; Oliver & Barnes, 2012) is also a concern:
Although materialism relies paradoxically on the liberal discourse of defending human rights, it fails to accommodate the individuality, pluralism, and diversity of disability experiences (Blackie, 2018; Owens, 2015; Turner & Blackie, 2018). Consequently, dissenters are often purged because, as Shakespeare and Watson (2001, p. 6) point out, “[y]ou can’t be a proper activist unless you accept the social model as your creed.” This characteristic also leads to a devaluation of all facts that challenge the “absolute truth” that change is an exclusive product of collective action, which in turn whitewashes the transformative force of individual paths taken by enterprising people and families who have completely escaped the institutional system and are the basis of most successful inclusion stories (Kleinfield, 1979a, 1979b; Levy, 1988).
Moreover, the rights-based approach to disability issues exacerbates rather than resolves the problems faced by disabled people (Owens, 2015). In current knowledge societies where non-formal knowledge recognition is low, the persistence of inequalities in terms of educational resources (EUROSTAT, 2019; Organization & Bank, 2011) and lack of control over installed supply, resulting from the characteristics of traditions that emerged from the 16thcentury, tend to diminish the impact of the principle “Nothing About Us Without Us”8 and exclude disabled people from the later stages of the political process, which are increasingly complex, scientific, and risk-averse (Douglas, 1986; King et al., 1994; Wegerich, 2001), despite good practices of consultation and involvement of civil society (Castells, 2010; Innerarity, 2012; Välimaa & Hoffman, 2008). This creates space for the emergence of hidden processes (Hacker et al., 2015; Thelen, 2003) that lead to the failure of institutional reform processes.
Finally, as this study has shown, the usefulness of the discourse of liberal capitalist (regimes) oppression is at best weak. Firstly, because patterns of exclusion and lack of power of disabled peoplepredate the 18th century, and secondly, because the existence of a planetary pattern of marginalization, institutional care, and lack of power of disabled people proves that it is not an exclusive product of liberal regimes (Organization & Bank, 2011). The 2019 report from the V-Dem Institute (V-Dem, 2019) on the quality of democracy in the world also shows that illiberal countries in terms of rights, freedom, and guarantees of their populations generally present discouraging results. Unfortunately, history shows that disabled people never was an exception to this reality (Amariei, 2003; Chikate, 2020; Parker & Clements, 2012; Phillips, 2009).
The social model influence has been noted in the internationalization process of disability issues, giving rise to a collection of national and international instruments that attempt to safeguard a set of rights and guarantees of disabled people, trying to influence their quality of life in different dimensions, and that influenced the doctrine that turns the defence of the rights of disabled people into a human rights issue (Barnes, 2019; Barnes & Mercer, 2010; Shakespeare, 2006).
One aspect that stands out in this internationalization is that it also reflects the tension (Das Gupta, 2001; Wegerich, 2001) that exists between the references of thought of a medical elite and a challenging sociological thought of an emerging elite of disabled thinkers and activists, which is evident in the revision process of the International Classification of Impairments, Disabilities, and Handicaps (ICIDH) that resulted in the International Classification of Functioning, Disability, and Health (ICF) and the emergence of a compromise model based on the biopsychosocial approach that, according to Owens (2015), has the Nordic version of the social model as its main inspiration.
The Independent Living Movement (ILM) is one of the approaches inspired by the social model that emerged in the United States, considering the high number of severely disabled people institutionalized whose degree of limitation makes them dependent on the assistance of others (DeJong, 1979b, 1979a; E. Roberts, 1989).
There is evidence that reveals an original matrix of the ILM that is distinct from the more normative character of the social/human rights model. Reading Pfeiffer (1988) gives the impression that some authors believe that realizing the lives of these individuals requires creating solutions that provide effective and facilitative responses for the full exercise of their right to participation. However, this distinction is becoming increasingly difficult to make, unfortunately in favour of normativity.
The emancipatory philosophy of the ILM sustains a set of principles that give it shape as a movement of action. According to some authors (DeJong, 1979b; Ratzka, 1989; Zola, 1988), these principles are empowerment, self-help, and peer counselling models, demedicalization, deinstitutionalization, deprofessionalization, control over representative organizations, absolute control over available services, and networking. As a systemic approach, it is based on a set of five facilitating elements: universal design (Oliveira, 2015), citizenship education (Oliveira, 2011), personal assistance and support services (Assembly, 2007; Standard Rules on the Equalization of
Opportunities for Persons with Disabilities : Resolution A/RES/48/96/ Adopted by the General Assembly, 1993), assistive products (Oliveira & Partidário, 2008), and financial supplements (tax benefits and direct payments) (Ratzka, 1989; Zarb & Nadash, 1994).
Now, a policy of support for independent living must be based on a strategy of articulated implementation of the five facilitating elements, respectful of the principles of the ILM, and focused on technical, financial, and informative support directed at the consumer. This implementation strategy has varied from country to country: in the United States, it focused on the role of Centres for Independent Living (CIL) as the primary coordinating organization through which disabled peopleengage in the awareness-raising and education activities necessary to meet their individual and collective objectives. In the Netherlands, the needs for support for independent living are met by crosscutting programs that combine a home care system with an independent living support system promoted by the health and social protection sectors (DeJong, 1984). In Denmark and Germany, support measures for independent living are associated with their main disability-directed social programs ((Jørgensen, 1982). In the UK, housing has been a key concern in the ILM strategy (Stewart et al., 1999).
The evidence shows that, in the medium/long term, there are a set of inherent advantages and benefits to the Independent Living paradigm in terms of education and job creation, social inclusion and participation of people in situations of dependence and their families, sustainability of social security systems, and the market (Barnes & British Council of Organizations of Disabled People, 1991; Berthoud et al., 1993; Morris, 1993; Zarb & Nadash, 1994; Zarb & Oliver, 1993).
In the 1970s and 1990s, many emancipatory models were notably influenced by the characteristics and values of the social model that played a crucial role in propelling disability activism. This influence led to significant achievements, including advocacy for anti-discrimination legislation, the campaign to legalize direct payments that empower disabled individuals to hire personal assistants, the establishment of integrated mechanisms for accessible housing (Parish & Braddock, 2001), and initiatives to redirect institutional resources towards community service activities (Covert et al., 1994).
While some countries continue to rely on institutional care (Mansell & Beadle-Brown, 2010), and there are challenges in obtaining accurate disability statistics for the institutionalized population (She & Stapleton, 2006), the majority of disabled individuals worldwide are not residing in institutions, mostly, thanks to the support of informal caregivers (OECD, 2017). However, it is important to note that the number of disabled people still living in institutions remains significant (Parker & Clements, 2012; Šiška & Beadle-Brown, 2020). This includes institutionalized disabled adults who often experience more severe and complex disabilities, such as intellectual, psychosocial, or multiple disabilities, compared to those living in the community (Fundamental Rights, 2017). Moreover, this group encompasses children with intellectual disabilities, autism, challenging behavior, as well as unaccompanied and separated migrant children (Šiška & Beadle-Brown, 2020).
Despite the gradual abandonment of large residential institutions and the development of smallscale community services being a reality on the political agenda in many countries, including Scandinavia, the United States, Canada, the United Kingdom, and Australasia (Okomayin & Ige, 2023; Yang et al., 2022), and these developments aligning with international legal frameworks (Mansell & Beadle-Brown, 2010), we are still at the early stages of an asymmetric institutional transition regarding the provision of social services that may not always be tailored to the needs and realities of consumers (Oliveira, 2023; Pinto, 2018).
Conclusion: Institutions, Power, and Institutional Change
Comparative historical analysis is a research method that involves comparing historical cases to understand patterns, processes, and causal relationships in social phenomena. It aims to identify similarities and differences between cases, analyse historical context, and examine how different factors interact to shape outcomes. This approach allows researchers to study long-term processes, trace historical trajectories, and make generalizations about social phenomena (Mahoney & Rueschemeyer, 2012; Skocpol, 1984a, 1984b).
Comparative historical analysis involves collecting and analysing qualitative and quantitative data from a range of sources, including archival records, interviews, and statistical data (Della Porta, 2008; King et al., 1994; Ragin, 2014). One of the central issues in comparative research is how to define and measure the variables of interest, in order to ensure the validity and reliability of the results. This implies choosing adequate units of analysis, criteria of selection and sampling, indicators and scales, sources and methods of data collection, techniques of analysis and interpretation (King et al., 1994).
In this scientific article, I constructed a visual representation illustrating the evolution of community living for disabled individuals across the studied periods in Chart 19. To achieve this, I categorized impairments into six groups: “Congenital physical impairments,” “Acquired physical impairments,” “Congenital sensory impairments,” “Acquired sensory impairments,” “Developmental impairments or mental illness,” and “Other impairments and diseases.”
Due to the lack of quantitative data, I have converted the non-numerical information from the cited bibliography, using a scale ranging from Total Absence (0) to Low-Medium Presence (1-5), High-Medium Presence (6-9), and Total Presence (10). This scale enables researchers to categorize and analyze data consistently, regardless of variations in disability types and historical contexts.
After evaluating each category across the nine time units, I computed the average for each time interval (“Antiquity,” “Biblical Societies,” “Low Middle Ages,” “High Middle Ages,” “Modern Age,” “18th century-1930,” “1930-1940,” “1940-1980,” and “1980-Present”) and have create chart 1.
Chart 1 – Evolution of the community living of disabled people
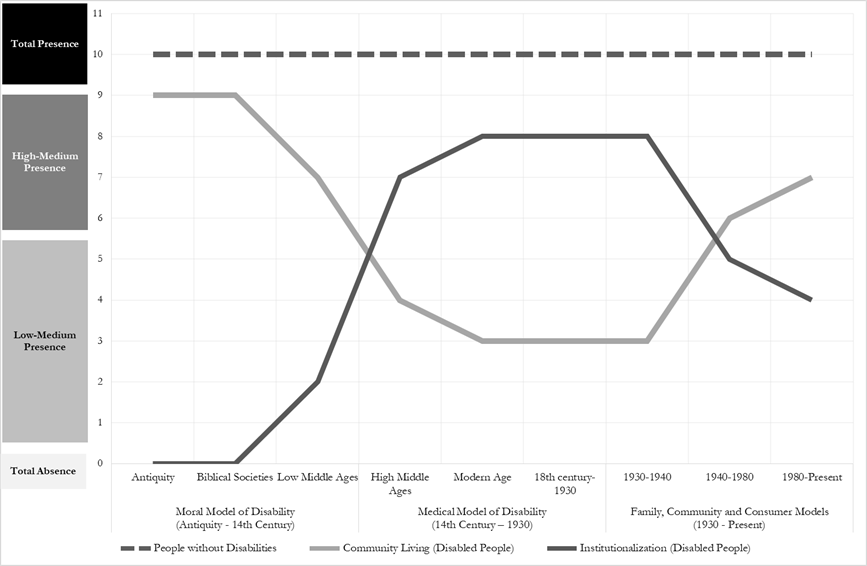
Source: Own elaboration based on the mentioned bibliography
Responding to the first question of this study, I will say that:
1. Is there variation among disability models in terms of attitudes and responses to the challenges and issues inherent in this social reality?
Using the ideal standard of community living, the pattern of community living of people without disabilities (total presence), a transversal reading of graph 1 reveals that the community living of disabled people in Antiquity and in Biblical Societies was almost complete (medium-high presence) due to the non-existence of institutional care and the socially accepted aspect of acquired disability. It is only not complete due the exposure of children with deformities in Ancient Greece and to home confinement and sanitary care for some disabled people.
This variation in how different types of disability are perceived, which still persists today, despite some ranking differences, explains why disabled people since Antiquity have been seen not only as the “Other,” but often as the “Other” of the “Other,” which explains the marginalization they are subject to, even by those who are equally marginalized (Clapton & Fitzgerald, 1997).
From the Late Middle Ages, a confirmed trend emerges, indicating the gradual distancing of disabled individuals from societal centres as institutional care progressively establishes itself (with a medium-low presence). The recapture of community space by disabled individuals only commenced from the mid-twentieth century (a continuous but gradual process, transitioning from medium-low presence to medium-high presence). Nevertheless, contemporary societies exhibit high levels of institutional care and technical demands within the labour market (Castells, 2010), which stand in contrast to the currently low levels of education among disabled individuals (EUROSTAT, 2019; Organization & Bank, 2011). These factors contribute to the generation of new and enhanced forms of social exclusion and isolation (Barnes, 2012). Consequently, it leads us to hypothesize that, proportionally, the community living and participation of disabled individuals in our societies is still less than that observed in Antiquity and Biblical Societies.
Based on this evidence, this article posits that despite a significant axiological shift in Western societal thinking about disability throughout the history, as demonstrated by the transition between disability models, the enduring exclusionary traditions persist, despite significant variations. This underscores the notion that the concept of invariance emerges as a defining characteristic of these traditions (Hobsbawm & Ranger, 1983). Consequently, not only is there a continual perpetuation of exclusionary, prejudiced, segregationist, and welfare-oriented patterns in the life experiences of disabled individuals across generations, impeding the realization of inclusive societies, but also the perpetuation of power disparities for disabled individuals.
Nevertheless, it can be argued that these models contribute to the understanding of crucial aspects in each historical period, including power relations among elites and the signalling of dominant references and ideas.
I now present Figure 1, which reflects, from a temporal perspective, the relationship between historical traditions and disability models.
Figure 1 – Temporal perspective of the relationship between historical traditions and models of disability
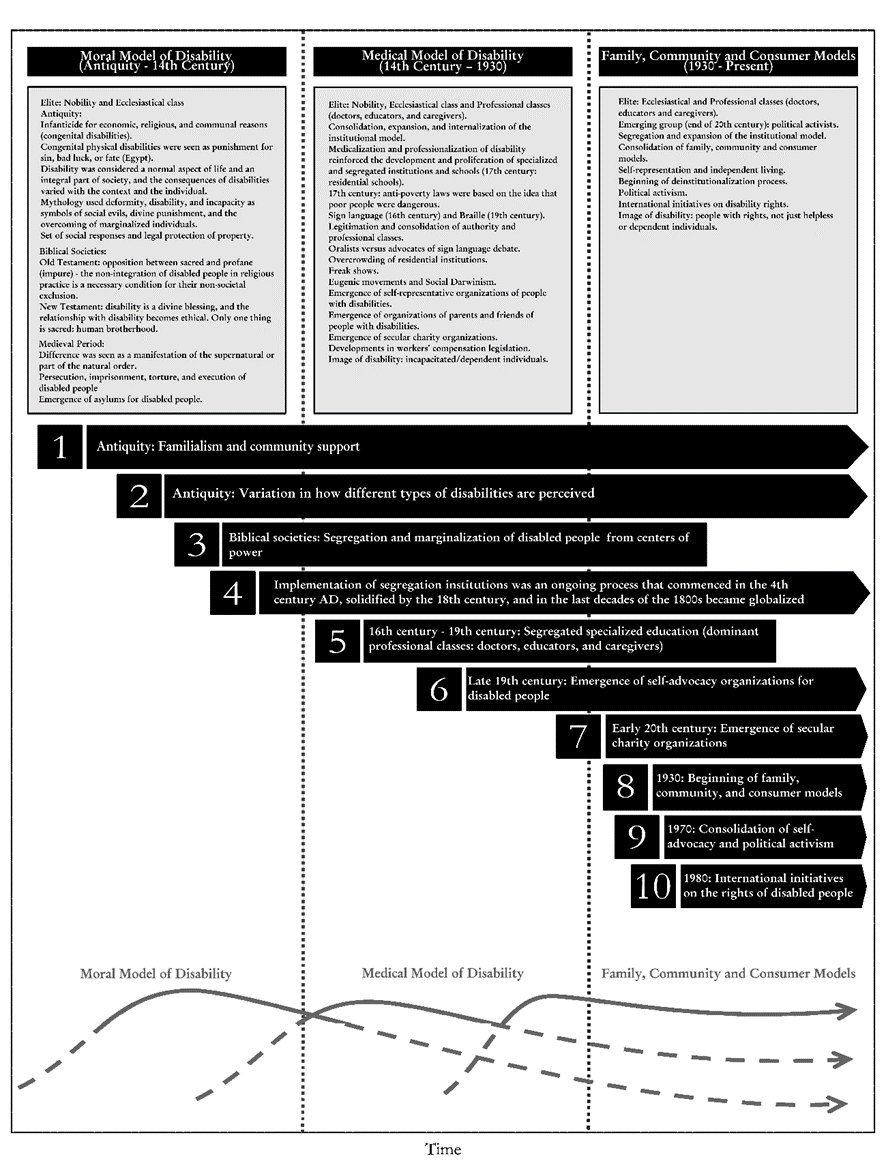
Source: Own elaboration based on the mentioned bibliography
Now responding to the second question of this study:
2. How has variation among disability models influenced the power dynamics of different actors involved and impacted the development and trajectories of political institutions?
Figure 1 illustrates that the community living of individuals with disabilities was a prevalent practice in ancient and biblical societies, showcasing a consistent historical tradition. From ancient Greece to biblical communities, the active engagement of disabled individuals within their communities persisted despite recommendations for home isolation in cases of mental disorders. Support primarily emanated from their families and communities (tradition 1).
In turn, the trend towards the progressive marginalization of disabled people from centres of power only began to be felt in biblical societies and as a direct consequence of the progressive assertion of segregationist norms (tradition 3). This segregationist tradition was reinforced with solutions for institutional care (tradition 4), beginning in the 4th century, and segregated specialized education (tradition 5), beginning in the 16th century. The peak of these three traditions was reached with the publication of the Poor Laws in England in 1601, which relied on the confinement of these people more because of their social status than their condition. Thus, of all the identified traditions, only traditions 3 and 5 were genuinely disrupted by the implementation of a collection of national and international legal instruments aimed at safeguarding the rights and guarantees of disabled people and influencing their quality of life in various dimensions.
Regarding the relationship between disability and access to power, despite the fact it is expected that many kings and emperors at least acquired it because of diseases and wars, the ecclesiastical and professional elites have shared power throughout the history to the detriment of the self-representation of disabled people.
This reality is evidenced by the strengthening of institutional care overtime that enable themaintenance of the Church work in the social sphere, often exclusively ensuring the fulfilment of the state’s social functions, especially in rural areas (Manow, 2015), and the rise of some professional classes of doctors, educators, and caregivers whose power would decisively determine the collective history of disabled people and would be legitimized and ensured by the replication of segregationist solutions, a practice that persists today (European Expert Group on the Transition from Institutional to Community-Based Care, 2014).
At the end of the 19th century, another important phenomenon emerged: the appearance of the first self-representative organizations of disabled people (tradition 6). The fact that the deaf and blind communities were the first groups to organize themselves in terms of self-representation is not a coincidence. This situation is closely related to the circumstance that social, technical, and technological advances allowed these people access to information and education before any other group of disabled people. This is explained by tradition 2.
In the mid-20th century, emancipatory models emerged and an elite of thinkers and activists with and without disabilities with challenging sociological thinking emerge. According to Parish & Braddock (2001), over a period of sixty years (1920-1980), we witnessed a linked and almost parallel process that began with the emergence of secular charity organizations, which played a precursor role in the development of the vocational rehabilitation movement (tradition 7) in a social support landscape that was previously dominated absolutely by religious charity. However, as they did not respond to a series of consumers’ needs, they led to the rise of associations of family and friends of disabled people (tradition 8) from the 1950s onwards, reaffirming the fundamental role of these actors, now with greater organizational capacity, who created community services.
These associations were fundamental in creating the window of opportunity for the crosssectional affirmation of self-representative organizations, which are the basis of current political activism (tradition 9), whose main reference is the social model that has driven, since the 1980s, the emergence of a collection of legal instruments, both national and international, that attempt to safeguard a set of rights and guarantees of disabled people and influence the quality of life of these people in different dimensions (tradition 10).
This reality highlights several key aspects:
Firstly, it underscores the analytical utility of disability models, but, from a neo-institutional perspective, confirms the low intensity and gradual nature of the disruption processes linked to these transitions. As shown in Figure 1, this situation demonstrates that models can be understood as cyclical waves of dominant values within political institutions, reflecting different geometries of power distribution among different political and professional elites.
Secondly, it suggests that the transformations instigated by mid-20th-century emancipatory movements challenging the status quo are not yet robust enough to overcome the resistance of most exclusionary traditions. Even knowing that some crucial structural factors and causal processes for political change are incremental, and considerable time lags may exist between the appearance of a causal factor and the occurrence of the result (Bonoli, 2007; Pierson, 2005, 2006), it would be important for emancipatory movements to realize that much of the power of the status quo relies on offering “easy solutions” that “solve problems” for policymakers.
As Acemoglu & Robinson (2008, p. 2) demonstrate when studying simultaneous change and persistence in institutions, “[i]n the baseline model, equilibrium changes in political institutions have no effect on the (stochastic) equilibrium distribution of economic institutions, leading to a particular form of persistence in equilibrium institutions, which we refer to as invariance. When the model is enriched to allow for limits on the exercise of de facto power by the elite in democracy or for costs of changing economic institutions, the equilibrium takes the form of a Markov regime-switching process with state dependence. Finally, when we allow for the possibility that changing political institutions are more difficult than altering economic institutions, the model leads to a pattern of captured democracy, whereby a democratic regime may survive but choose economic institutions favoring the elite.”
Indeed, similar to economic institutions, due to the dominance in the provision of social services, the change in dominant values within political institutions may not necessarily signify a permanent departure from past practices related to disability. This also justifies the persistence of certain morally inclined ideals associated with disability, or the enduring significance of the medical model values, even in contemporary times dominated by the doctrine of the human rights model. Finally, it highlightsthe evident continuous nature of history and the tension between processes of change and the interests of elites during the transition between models (Das Gupta, 2001; Wegerich, 2001).
So, to accomplish change, I believe that the next stage of emancipatory movements’ seems to bemore focused on building and control sustainable solutions supported on an narrative capable of dispel the spectre of risk and uncertainty inherent in change, than on advocating for change, knowing thatwhen faced “… with uncertainties, cautious policymakers prefer the known difficulties of the status quo to the risks of adopting a new Programme” (R. Rose, 2005, p. 127).
Thirdly, the prolonged periods of marginalization, segregation, and disempowerment of disabled individuals significantly challenge the discourse against the oppression of the liberal capitalist regime. The notion that economic changes, particularly industrialization, marginalized disabled people in the workforce should be critically examined and substantiated through comparative studies analyzing various economic sectors, regions, nations, and periods. Such analyses would enhance our understanding of the repercussions of economic change on disabled individuals.
Notes
1 Research carried out with the support of the Foundation for Science and Technology (FCT).
2 PhD Political Science – specialization in Political Institutions and Processes.
3 In this research, I adopt a definition of axiological rupture that characterizes it as a radical and forceful form of discontinuity in values or beliefs. Explored across various contexts (Holbraad et al., 2019; Kingsmith, 2017), axiological rupture can instigate significant shifts in societal and individual perspectives,often manifesting in protests, violence, or the quest for new forms of identity and meaning (Portela, 2017).The concept challenges the conventional notion of continuity and underscores the critical dimension of change in both social theory and public discourse (Richman & Lemons, 2023).
4 Conceptual models often act as abstractions of real-world entities, encompassing both physical and social aspects (Tatomir et al., 2018). Consequently, the disability model refers to various frameworks or perspectives through which disability is comprehended and addressed in Western societies. These models influence how society perceives and responds to disability (Retief & Letšosa, 2018).
5 According to Parish & Braddock (2001), the most negative perspective was developed by historians of the 19th century who applied their contemporary contempt for disabled people to their evaluation of the ancient world.
6 https://www.biblegateway.com/passage/?search=Leviticus%2013&version=ESV
7 The 1840 census reflected widespread racism, as all Black residents were classified as insane, leading to an exponential increase in the population with disabilities.
8 Principle and slogan of the international disability rights movement.
9 It is important to highlight that, from my perspective, a substantial degree of community integration for disabled individuals does not inherently result in heightened levels of inclusion or increased participation. Merely being present in the community does not automatically translate into enhanced inclusion or active engagement for disabled individuals. Through my observations and experience, I have noted that, even when living outside institutional settings, many disabled people experience minimal or non-existent levels of social inclusion and participation. This reality spans various scenarios, including instances where disabled individuals encounter challenges related to employment, face limitations in educational attainment, or have restricted social connections, among other examples.
Acknowledgment
I would also like to thank Professor Belén Rando for the final revision and Professor David Camocho for redesigning the figures and graphics presented in this article.
Bibliography
Acemoglu, D., & Robinson, J. A. (2008). Persistence of power, elites, and institutions. American Economic Review, 98(1), 267–293.
Adair, R., Melling, J., & Forsythe, B. (1997). Migration, family structure and pauper lunacy in Victorian England: Admissions to the Devon County Pauper Lunatic Asylum, 1845–1900.
Continuity and Change, 12(3), 373–401.
Amariei, R. (2003). Romania: Including the excluded. How a Self-Help Initiative Proved That Institutionalization and Exclusion Are Not the Only Options for the Intellectually Disabled. Retrieved July, 2, 2006.
Andrews, J. (1998). Begging the question of idiocy: The definition and socio-cultural meaning of idiocy in early modern Britain: Part 1. History of Psychiatry, 9(33), 65–95.
Assembly, U. N. G. (2007). Convention on the Rights of Persons with Disabilities: Resolution / adopted by the General Assembly (Vol. 61, Issue 106).
https://www.refworld.org/docid/45f973632.html
Axinn, J., & Levin, H. (1982). Social Welfare: A History of the American Response to Need. Harper & Row. https://books.google.pt/books?id=ENUPAQAAMAAJ
Barnes, C. (2012). Re‐thinking disability, work and welfare. Sociology Compass, 6(6), 472–484.
Barnes, C. (2019). Understanding the social model of disability: Past, present and future. In Routledge handbook of disability studies (pp. 14–31). Routledge.
Barnes, C. & British Council of Organizations of Disabled People. (1991). Disabled People in Britain and Discrimination: A Case for Anti-discrimination Legislation. C. Hurst & Company. https://books.google.pt/books?id=uDiyAAAAIAAJ
Barnes, C., & Mercer, G. (2010). Exploring Disability. Polity Press.
https://books.google.pt/books?id=V7qJlWqcbrcC
Barnes, C., & Oliver, M. (1993). Disability: A sociological phenomenon ignored by sociologists. University of Leeds Leeds.
Berg, M., & Hudson, P. (1992). Rehabilitating the industrial revolution. The Economic History Review, 45(1), 24–50.
Berthoud, R., Lakey, J., & McKay, S. (1993). The Economic Problems of Disabled People.
https://www.semanticscholar.org/paper/The-Economic-Problems-of-Disabled-PeopleBerthoud-Lakey/ddbb9d7aa47d37f3a8fa66dbb692db6ac66cac6
Blackie, D. (2018). Disability and work during the industrial revolution in Britain. In The Oxford Handbook of Disability History(pp. 177–193). Oxford University Press.
Bogdan, R. (1988). Freak show: Presenting human oddities for amusement and profit. University of Chicago Press.
Bonoli, G. (2007). Time matters: Postindustrialization, new social risks, and welfare state adaptation in advanced industrial democracies. Comparative Political Studies, 40(5), 495–520.
Braddock, D. (1986). Federal assistance for mental retardation and developmental disabilities I: A review through 1961. Mental Retardation, 24(3), 175.
Castells, M. (2010). The Rise of the Network Society: The Information Age: Economy, Society, and Culture. Wiley. https://books.google.pt/books?id=62FPnwEACAAJ
Cavallo, S. (2013). Family obligations and inequalities in access to care in northern Italy, seventeenth to eighteenth centuries. In The Locus of Care(pp. 90–110). Routledge.
Chikate, P. (2020). Disabled women in a dictatorial regime: Sexual assault and disability in Zimbabwe.Minnesota State University, Mankato.
Clapton, J., & Fitzgerald, J. (1997). The history of disability: A history of’otherness’. New Renaissance Magazine, 7(1), 1–3.
Colón, D. M. (1989). Martin Luther, the devil and the teufelchen: Attitudes toward mentally retarded children in sixteenth-century Germany. Proceedings of the PMR Conference, 14, 75–84.
Corker, M. (1999). Differences, Conflations and Foundations: The limits to ‘accurate’ theoretical representation of disabled people’s experience? Disability & Society, 14(5), 627–642.
https://doi.org/doi:10.1080/09687599925984
Corker, M. (2002). Deafness/disability – problematising notions of identity, culture, and structure(S. Ridell & N. Watson, Eds.). Pearson.
Covey, H. C. (1998). Social Perceptions of People with Disabilities in History. Charles C Thomas.
Crow, L. (1996). Including all our lives: Renewing the social model of disability (J. Morris, Ed.). Women’s Press.
Daniels, M. (1997). Benedictine Roots in the Development of Deaf Education: Listening with the Heart. Bergin & Garvey.
Das Gupta, M. (2001). State-Community Synergies in Development: Laying the basis for collective action, World Bank. Development Research Group.
Davis, L. (1997). The Disability Studies Reader. Routledge.
DeJong, G. (1979a). Independent Living: From Social Movement to Analytic Paradigm”. Archives of Physical Medicine and Rehabilitation, 60, 435–446.
DeJong, G. (1979b). The Movement for Independent Living: Origins, Ideology, and Implications for Disability Research. University Center for International Rehabilitation, Michigan State University.
DeJong, G. (1984). Independent Living and Disability Policy in the Netherlands: Three Models of Residential Care and Independent Living. International Exchange of Experts and Information in Rehabilitation, World Rehabilitation Fund.
Delcourt, M. (1986). Stérilités mystérieuses et naissances maléfiques dans l’Antiquité classique. les Belles lettres. https://books.google.pt/books?id=p-uCoAEACAAJ
Della Porta, D. (2008). 11 Comparative analysis: Case-oriented versus variable-oriented research.
Approaches and Methodologies in the Social Sciences, 198.
Douglas, M. (1986). How institutions think. Syracuse University Press.
Edwards, M. L. (1996). The Cultural Context of Deformity in the Ancient Greek World. Ancient History Bulletin, 10, 79–92.
Edwards, M. L. (1997). Deaf and Dumb in Ancient Greece”. In L. Davis (Ed.), The Disability Studies Reader. Routledge.
Erevelles, N. (2001). In search of the disabled subject. In Embodied rhetorics: Disability in language and culture(pp. 92–111).
European Expert Group on the Transition from Institutional to Community-based Care. (2014).
EUROSTAT. (2019). Archive: Disability statistics—Access to education and training. Statistics Explained. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Archive:Disability_statistics_-_access_to_education_and_training&oldid=399898.
Farmer, S. (1998). Down and Out and Female in Thirteenth Century Paris”. American Historical Review, 103, 344–372.
Finkelstein, V. (1980). Attitudes and Disability: Issues for Discussions. World Rehabilitation Fund.
Finklestein, V. (2001). A personal journey into disability politics.
Foucault, M. (1973). Madness and Civilization: A History of Insanity in the Age of Reason. Vintage Books. https://books.google.pt/books?id=6uc2AQAAIAAJ
Fundamental Rights, E. U. A. (2017). Summary overview of types and characteristics of institutional and community-based services for persons with disabilities available across the EU.
https://fra.europa.eu/sites/default/files/fra_uploads/2017-10-independent-living-mappingpaper_en.pdf
Garland, R. (1995). The eye of the beholder: Deformity and disability in the Graeco-Roman world. Cornell University Press.
Girard, R. (1972). La violence et le sacré. Grasset.
Girard, R. (2001). Des choses cachées depuis la fondation du monde.
Gleeson, B. (1999). Geographies of disability. Psychology Press.
Grob, G. N. (1994). The Mad among Us. Free Press.
Hacker, J. S., Pierson, P., & Thelen, K. (2015). Drift and conversion: Hidden faces of institutional change. Advances in Comparative-Historical Analysis, 180–208.
Hobsbawm, E., & Ranger, T. (Eds.). (1983). The invention of tradition. Cambridge University Press.
Holbraad, M., Kapferer, B., & Sauma, J. F. (2019). Ruptures: Anthropologies of discontinuity in times of turmoil. UCL Press.
Hughes, B. (1999). The constitution of impairment: Modernity and the aesthetic of oppression. Disability and Society, 14, 2, 155–172.
Hughes, B., & Paterson, K. (1997). The social model of disability and the disappearing body: Towards sociology of impairment. Disability and Society, 12, 3, 325–340.
Imrie, R. (1997). Rethinking the relationships between disability, rehabilitation and society. Disability and Rehabilitation, 19, 7, 263–271.
Innerarity, D. (2012). Power and knowledge: The politics of the knowledge society. European Journal of Social Theory, 16(1), 3–16.
Jankauskas, R., & Urbanavicius, A. (1998). Diseases in European Historical Populations and Their Effects on Individuals and Society”. Collegium Antropologicum, 22, 465–476.
Jones, L. A. (1987). Doing Justice: A History of the Association of Retarded Citizens of Washington. The Arc of Washington.
Jørgensen, S. (1982). Independent Living for Handicapped Persons in Denmark”. In D. G. Tate & L. M. Chadderdon (Eds.), Independent Living: An Overview of Efforts in Five Countries (pp.11–29). University Center for International Rehabilitation, Michigan State University.
King, G., Keohane, R. O., & Verba, S. (1994). Designing Social Inquiry: Scientific Inference in Qualitative Research.
Kingsmith, A. (2017). On rupture: An intervention into epistemological disruptions of Machiavelli, Hobbes, and Hume. JSP: Journal of Speculative Philosophy, 31(4), 594–608.
Kleinfield, S. (1979a). Declaring independence in Berkeley”. Psychology Today.
Kleinfield, S. (1979b). The hidden minority.Atlantic-Little, Brown.
Lane, H. (1989). When the Mind Hears: A History of the Deaf. Random House.
Lang, R. (2001). THE DEVELOPMENT AND CRITIQUE OF THE SOCIAL MODEL OF DISABILITY.
Lefley, H. (1996). Family Caregiving in Mental Illness. Sage.
Levy, C. W. (1988). A people’s history of the independent living movement. The Research and Training Center on Independent Living, University of Kansas.
Linton, S. (1998). Claiming Disability: Knowledge and Identity. New York University Press.
Longmore, P. (2003). Why I burned my book (Vol. 12). Temple University Press.
Mahoney, J., & Rueschemeyer, D. (2012). Comparative historical analysis: Achievements and agendas. In Comparative Historical Analysis in the Social Sciences (pp. 3–38).Cambridge University Press.
Manow, P. (2015). Workers, Farmers and Catholicism: A History of Political Class Coalitions and the South-European Welfare State Regime. Journal of European Social Policy, 25(1), 32–49.
Mansell, J., & Beadle-Brown, J. (2010). Deinstitutionalisation and community living: Position statement of the comparative policy and practice special interest research group of the international association for the scientific study of intellectual disabilities. Journal of Intellectual Disability Research, 54(2), 104–112.
March, J. G., & Olsen, J. P. (2006). Elaborating the ‘new institutionalism’. The Oxford Handbook of Political Institutions, 5, 3–20.
Marks, D. (1999). Dimensions of Oppression: Theorising the Embodied Subject”. Disability & Society, 14(5), 661–626.
Miles, M. (2000). Signing in the Seraglio: Mutes, Dwarfs and Jestures at the Ottoman Court 1500-1700”. Disability & Society, 15(1), 115–134.
Morris, J. (1993). Independent Lives? Community Care and Disabled People. Macmillans.
OECD. (2017). Health at a Glance 2017: OECD Indicators. Organisation for Economic Cooperation and Development. https://www.oecd-ilibrary.org/social-issues-migrationhealth/health-at-a-glance-2017_health_glance-2017-en
Okomayin, A., & Ige, T. (2023). Ambient Technology & Intelligence. arXiv Preprint arXiv:2305.10726.
Oliveira, P. N. de. (2023). Assistência Pessoal e Desfamiliarismo: Um Teste Prático ao Modelo de Apoio à Vida Independente Português.
Oliveira, P. N. (2011). O Movimento Vida Independente e a história da inclusão: Reflexos sociocomunicacionais de conquista, tecnologia, empreendedorismo e Inovação. Notas introdutórias. In Comunicar e Interagir: Um Novo Paradigma para o Direito à Participação Social das Pessoas com Deficiência.
Oliveira, P. N. (2015). Políticas Públicas, Inovação e Cidadania: O Sistema Prometheus. FCSH/UNL.
Oliveira, P. N., & Partidário, P. J. (2008). Que oportunidade para inovação sustentável no Sistema Nacional de Atribuição das Ajudas Técnicas/Tecnologias de Apoio?”. Revista de Educação Especial e Reabilitação. Edições FMH-UTL, 14, 15–49.
Oliver, M. (1983). Social Work with Disabled People. Macmillan.
Oliver, M. (1990). The Politics of Disablement. Macmillan.
Oliver, M. (1996). Understanding Disability: From Theory to Practice. Macmillan.
Oliver, M., & Barnes, C. (2012). The new politics of disablement. Macmillan International Higher Education.
Organization, W. H., & Bank, W. (2011). World report on disability. World Health Organization.
Owens, J. (2015). Exploring the critiques of the social model of disability: The transformative possibility of Arendt’s notion of power. Sociology of Health & Illness, 37(3), 385–403.
Parish, S. L., & Braddock, D. (2001). An Institutional History of Disability. In Gary L. Albrecht, Katherine D. Seelman, & Michael Bury (Eds.), Handbook of Disability (pp. 11–68). Sage Publications.
Parker, C., & Clements, L. (2012). The European Union Structural Funds and the right to community living.
Pfeiffer, D. (1988). Divisions in the disability community”. Department of Sociology.
Phillips, S. D. (2009). ‘ There are no invalids in the USSR!’ A missing Soviet chapter in the new disability history. Disability Studies Quarterly, 29(3).
Pierson, P. (2005). The study of policy development”. Journal of Policy, istory,17(01), 34–51.
Pierson, P. (2006). Public policies as institutions”. In Rethinking political institutions: The art of the state (pp. 114–131).
Pierson, P., & Skocpol, T. (2002). Historical institutionalism in contemporary political science’. In I.
Katznelson & H. V. Miller (Eds.), Political Science: State of the Discipline (pp. 693–721). Norton.
Pinto, P. C. (2018). From rights to reality: Of crisis, coalitions, and the challenge of implementing disability rights in Portugal. Social Policy and Society, 17(1), 133–150.
Plann, S. (1997). A Silent Minority: Deaf Education in Spain, 1550-1835. University of California Press.
Portela, I. (2017). A ruptura epistemológica entre a globalização da economia de mercado e a globalização do regionalismo latino-americano e do brasil: Qual é o espaço do cidadão? Revista Juridica, 3(48), 1–13.
Ragin, C. C. (2014). The comparative method: Moving beyond qualitative and quantitative strategies. Univ of California Press.
Ratzka, A. (1989). Personal Assistance as Key to Independent Living. In Keynote). ENIL – European Network on Independent Living.
Retief, M., & Letšosa, R. (2018). Models of disability: A brief overview. HTS Teologiese Studies/Theological Studies, 74(1).
Rhodes, R. A. W., Binder, S. A., & Rockman, B. A. (2006). The Oxford handbook of political institutions. Oxford University Press Oxford; WorldCat.
Richards, P. L. (2009). Industrialization. In S. Burch (Ed.), Encyclopedia of American Disability History (Vol. 3, p. 482-3). Facts on File.
Richman, N., & Lemons, J. D. (2023). Introduction: From rupture to repair.
Roberts, E. (1989). A History of the Independent Living Movement: A Founder’s Perspective”. In B.
W. Heller, L. M. Flohr, & L. S. Zegans (Eds.), Psychosocial Interventions with Physically Disabled Persons (pp. 231–244). Rutgers University Press.
Roberts, F. K. (1986). Education of the Visually Handicapped: A Social and Educational History”.
Foundations of Education for Blind and Visually Handicapped Children and Youth: Theory and Practice (G. T. Scholl, Ed.). American.
Rockey, D. (1980). Speech Disorder in Nineteenth Century Britain. Croom Helm.
Rose, R. (2005). Learning from comparative public policy: A guide to lesson-drawing. Routledge.
Rose, S. F. (2017). No right to be idle: The invention of disability, 1840s–1930s. UNC Press Books.
Rothfels, N. (1996). Aztecs, Aborigines, and ApePeople: Science and Freaks in Germany, 1850-1900”. In R. G. Thomson (Ed.), Freakery: Cultural Spectacles of the Extraordinary Body(pp. 158–172). New York University Press.
Rothman, D. J. (1990). The Discovery of the Asylum: Social Order and Disorder in the New Republic (Rev.). Little.
Rushton, P. (1988). Lunatics and Idiots: Mental Disability, the Community, and the Poor Law in North-East England, 1600-1800. Medical History, 32, 34–50.
Rushton, P. (1996). Idiocy, the Family, and the Community in Early Modern Northeast England”. In D. Wright & A. Digby (Eds.), From Idiocy to Mental Deficiency: Historical Perspectives on People with Learning Disabilities (pp. 44–64). Routledge Kegan Paul.
Scull, A. (1991). Psychiatry and Social Control in the Nineteenth and Twentieth Centuries”. History of Psychiatry, 2, 149–169.
Shakespeare, T. (1994). Cultural representations of disabled people: Dustbins for disavowal.
Disability and Society, 9, 3, 283–299.
Shakespeare, T. (2006). Disability Rights and Wrongs. Routledge.
Shakespeare, T., & Watson, N. (2001). The social model of disability: An outdated ideology?
Research in Social Science and Disability, 2, 9–28.
She, P., & Stapleton, D. C. (2006). An Inventory of Disability Information for the Population Living in Institutions.
Šiška, J., & Beadle-Brown, J. (2020). Report on the transition from institutional care to communitybased services in 27 EU member states. European Expert Group on Transition from Institutional to Community-Based Care.
Skocpol, T. (1984a). 11. Emerging Agendas and Recurrent Strategies in Historical Sociology. Vision and Method in Historical Sociology, 356.
Skocpol, T. (1984b). Sociology’s historical imagination. Vision and Method in Historical Sociology, 8.
Standard Rules on the Equalization of Opportunities for Persons with Disabilities : Resolution A/RES/48/96/ Adopted by the General Assembly, U.N.General Assembly, Volume: 48 (1993). https://www.refworld.org/docid/3b00f2e80.html
Stewart, J., Harris, J., & Sapey, B. (1999). Disability and Dependency: Origins and Futures of ‘Special Needs’ Housing for Disabled People”. Disability and Society, 14, 5–20.
Stiker, H. J. (1997). A history of disability. University of Michigan Press.
Suzuki, A. (1991). Lunacy in Seventeenth and Eighteenth Century England: Analysis of Quarter Sessions Records. Part I”. History of Psychiatry, 2, 437–456.
Switzky, H. N., Dudzinski, M., Acker, R., & Gambro, J. (1988). Historical Foundations of OutofHome Residential Alternatives for Mentally Retarded Persons”. Integration of Developmentally Disabled Individuals into the Community (L. W. Heal, J. I. Haney, & A. R.
N. Amado, Eds.; 2d ed.). Brookes.
Tatomir, A., McDermott, C., Bensabat, J., Class, H., Edlmann, K., Taherdangkoo, R., & Sauter, M.
(2018). Conceptual model development using a generic Features, Events, and Processes(FEP) database for assessing the potential impact of hydraulic fracturing on groundwater aquifers. Advances in Geosciences, 45, 185–192. https://doi.org/10.5194/adgeo-45-185-2018
Terzi, L. (2004). The social model of disability: A philosophical critique. Journal of Applied Philosophy, 21, 2, 141–157.
Thelen, K. (2003). How Institutions Evolve: Insights from Comparative Historical Analysis.
Comparative Historical Analysis in the Social Sciences, 208–240.
Thomson, R. G. (1996). Freakery: Cultural Spectacles of the Extraordinary Body. New York University Press.
Thomson, R. G. (1997). Extraordinary Bodies: Figuring Physical Disability in American Culture and Literature. Columbia University Press.
Trent, J. W. (1995). Inventing the Feeble Mind: A History of Mental Retardation in the United States. University of California Press.
Turner, D. M., & Blackie, D. (2018). Disability in the Industrial Revolution: Physical impairment in British coalmining, 1780-1880. Manchester University Press.Välimaa, J., & Hoffman, D. (2008). Knowledge society discourse and higher education”. Higher Education, 56(3), 265–285.
V-Dem. (2019). Democracy Facing Global Challenges: V-Dem Annual Democracy Report 2019. VDem Institute.
von Beyme, K. (2006). Political Institutions: Old and New. In R. A. W. Rhodes, S. A. Binder, & B.
A. Rockman (Eds.), The Oxford handbook of political institutions. Oxford University Press Oxford; WorldCat.
Wegerich, K. (2001). Institutional change: A theoretical approach. Occasional Paper, 30.
Williams, S. J. (1999). Is anybody there? Critical realism, chronic illness and the disability debate.
Sociology of Health & Illness, 21, 6, 797–819.
Winzer, M. A. (1993). The History of Special Education: From Isolation to Integration. Gallaudet University Press.
Yang, G., Wan, L., Dong, H., Liang, X., & He, Y. (2022). Utilisation willingness for institutional care by the disabled elderly and its influencing factors based on Andersen’s model: A crosssectional survey of Henan, China. BMJ Open, 12(12)Zarb, G., & Nadash, P. (1994). Cashing in on Independence: Comparing the Cost and Benefits of Cash and Services for Meeting Disabled People’s Support Needs. Policy Studies Institute for the British Council of Organisations of Disabled People.
https://books.google.pt/books?id=AJr-vQEACAAJ
Zarb, G., & Oliver, M. (1993). Ageing with a Disability: What do they expect after all these years?University of Greenwich.
Zola, I. K. (1988). The Independent Living Movement: Empowering People With Disabilities”.
Australian Disability Review, 1, n.o 3.