Living with an Intractable Disease: Technology and “Technical Peer Support” for an ALS Patient
Tomoo HIDAKA*
*Graduate School of Letters, Ritsumeikan University, Japan Society for the Promotion of Science Research Fellow
1. Introduction
Amyotrophic lateral sclerosis (ALS), also referred to as Lou Gehrig’s disease in the United States, is a progressive, incurable motor neuron disease. It has afflicted many famous figures, including theoretical physicist and cosmologist Dr. Stephen William Hawking. Patients gradually lose body function because of the degeneration of motor neurons. With time, patients encounter difficulty in speaking and eventually require a respirator after the loss of spontaneous breathing. Nonetheless, there are differences in the progress of the disease, and this can be a problematic issue. On average, patients begin using a respirator three years after the initial diagnosis, although some patients require it after only a year. However, their consciousness, intelligence, and perception are nonetheless unimpaired. These patients therefore need another way to communicate in order to live within an unmoving body.
Techniques and technologies for effective communication have been developed for the people who face difficulties in communication, including ALS. These are often included in assistive technology. There are many kinds of support tools such as the word plate and nurse call. It is important for patients not only to respond to a life-threatening condition but to also share their experience and conduct advocacy-related work on behalf of other ALS patients. Some patients have communicative aids to write a book or report their experience to the general public as a form of patient advocacy work. The communicative capacity of the patients can be developed using these technologies.
Nonetheless, there are problems with the continuous use of assistive technology. One problem is the lack of skillful supporters who are knowledgeable about both the disease and the related technology. Research specifically shows that one-third of assistive technology is abandoned within three months because of the lack of effective patient support (Lasker and Bedrosian, 2000). On the other hand, in a few exceptional cases, patients have been able to continuously use assistive technology with the help of a supporter.
In this study, I focused on an example that includes two individuals. The first is Mr. Wanaka, an ALS patient known for his active involvement in patient advocacy activities; at home, he uses his cheek for communication and receives 24-hour care. The second is Mr. Hisazumi, an ALS patient supporting other patients’ communication through his knowledge of information technology.
This background led to our basic research question: “How does Mr. Wanaka live in this manner?” Therefore, the following two issues should be examined. The first is clarifying the actual condition of the home care Mr. Wanaka receives. The second is an understanding of the unique technology created by Mr. Wanaka and Mr. Hisazumi on the basis of the particularity of the home, including differences in the patients’ home themselves and differences in the effective support received.
2. Method
The participants were directly observed at Mr. Wanaka’s home 13 times in a month between August 4, 2007, and January 26, 2009. The involved people were Mr. Wanaka, other members of the Wanaka family, his caregiver, Mr. Hisazumi, and Mr. Hisazumi’s caregiver. Data were collected using focused question interviews and observations. Dr. Shodo Mizuki, a co-researcher, was included in this fieldwork.
3. Result and Discussion
3-1. Overview of Mr. Wanaka’s Home Care
The results are summarized in six scenes depicted in Figures 1–4.
 Figure 1 shows Mr. Wanaka’s bed. The basic structure of Mr. Wanaka’s house is common in Japan, although there are some unfamiliar aspects. Computers (Mac and PC) and communication aids were placed in front of his bed. A respirator was also placed at the back of the bed.
Figure 1 shows Mr. Wanaka’s bed. The basic structure of Mr. Wanaka’s house is common in Japan, although there are some unfamiliar aspects. Computers (Mac and PC) and communication aids were placed in front of his bed. A respirator was also placed at the back of the bed.
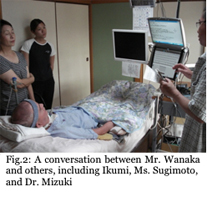 Figure 2 shows a conversation between Mr. Wanaka, his wife (Ikumi), his caregiver (Ms. Sugimoto), and Dr. Mizuki[1]. Here, Mr. Wanaka uses communication aids to speak with others, and sometimes, winks to answer “Yes”/”No” questions. This figure also depicts Ms. Sugimoto adjusting the position of Mr. Wanaka’s left hand (into which one of the interface tools was placed). She specifically asked “Is this the best position for you?,” and he answered the question with a wink, including cheek movements. The basic signs for “Yes”/”No” questions were previously decided between Mr. Wanaka and his caregivers, including Ms. Sugimoto. He does not always need to use computers for communication and can respond quickly to “Yes”/”No” questions.
Figure 2 shows a conversation between Mr. Wanaka, his wife (Ikumi), his caregiver (Ms. Sugimoto), and Dr. Mizuki[1]. Here, Mr. Wanaka uses communication aids to speak with others, and sometimes, winks to answer “Yes”/”No” questions. This figure also depicts Ms. Sugimoto adjusting the position of Mr. Wanaka’s left hand (into which one of the interface tools was placed). She specifically asked “Is this the best position for you?,” and he answered the question with a wink, including cheek movements. The basic signs for “Yes”/”No” questions were previously decided between Mr. Wanaka and his caregivers, including Ms. Sugimoto. He does not always need to use computers for communication and can respond quickly to “Yes”/”No” questions.
 Figure 3 shows the cheek interface created by Mr. Hisazumi. It was made from a combination of easy-to-find, inexpensive everyday materials, through the dialogue between Mr. Wanaka and Mr. Hisazumi (Fig.3). Thus, the materials used for the interface were not uncommon. Here, the two people have a dialogue about the usability of the interface and how it can be made better. Making better interfaces is not an easy task because the patient’s sensations are difficult to measure.
Figure 3 shows the cheek interface created by Mr. Hisazumi. It was made from a combination of easy-to-find, inexpensive everyday materials, through the dialogue between Mr. Wanaka and Mr. Hisazumi (Fig.3). Thus, the materials used for the interface were not uncommon. Here, the two people have a dialogue about the usability of the interface and how it can be made better. Making better interfaces is not an easy task because the patient’s sensations are difficult to measure.
 Figure 4 depicts communication with other patients via the Internet through instant messenger. This method is also used to attend remote meetings and lectures. Mr. Wanaka uses communication aids, a Macintosh, and a PC, through the interface. For example, he often exchanges information regarding home care techniques with other patients. He also uses this telecommunication system to attend remote meetings and lectures for patient advocacy. In this way, he remains active even though he is at home.
Figure 4 depicts communication with other patients via the Internet through instant messenger. This method is also used to attend remote meetings and lectures. Mr. Wanaka uses communication aids, a Macintosh, and a PC, through the interface. For example, he often exchanges information regarding home care techniques with other patients. He also uses this telecommunication system to attend remote meetings and lectures for patient advocacy. In this way, he remains active even though he is at home.
3-2. Characteristics of the “Technical Peer Supporter”
These results imply that Mr. Hisazumi has played an important role in providing and maintaining home care for Mr. Wanaka, especially through his technical support activities. The following three points effectively summarize the characteristics of this “technical peer supporter.”
First, the role of the “technical peer supporter” is not simply to be a “peer” but also a creator of customized technology. Second, there was also a process of perfection. In the present case, there was a specific dialogue between Mr. Wanaka and Mr. Hisazumi, who became agents of technology creation and use through the sharing of their experiences. Third, the destination of the support, referred to as “addressivity” (Bakhtin, 1986) was also notable. They knew who the user and the creator were, maintaining a dialogue that enabled Mr. Hisazumi’s support to continue.
On the basis of these discussions, Mr. Hisazumi may perhaps be best described as a “reflective practitioner” (Schon, 1983) with local knowledge. He improves the home care environment with the customization of everyday materials and constantly searches for the better solution.
4. Conclusion
In conclusion, technical peer support is based on “addressivity,” which makes for an on-going interactive relationship that can create the best technology for each individual. It contrasts strongly with modern bulk production methods. Mr. Hisazumi’s technology has a clear user and a creator, and it provides support suitable for each individual patient. Mr. Hisazumi considers his activity a key source of motivation in life. Thus, understanding Mr. Hisazumi’s perspective is an interesting issue.
On the other hand, it is also important to mention that the relationship between Mr. Wanaka and Mr. Hisazumi is based on the network and activities of the patients’ group. There are historical and relational backgrounds related to this aspect. The computers and respirators were also provided through social and financial support systems of the society.
If one applies this case to another patient, one needs to study these backgrounds. This may still seem difficult to apply because of its particularity. However, it is more important that communication support is realized in the field. This will act as a good starting point for studying technology, support activities, and health care.
[1] In this study we used the autonyms of the involved people, to describe the patient’s life as actual person’s one. It was a requirement from them, and all of photographs and autonyms in this study have been allowed to use through the full consultation with them.
5. References
- Bakhtin, M. M. (1986). Speech genres and other late essays. C. Emerson & M. Holquist, (Eds.) Austin, TX: University of Texas Press.
- Lasker, J. P., & Bedrosian, J. L. (2000) Acceptance of AAC by adults with acquired disorders. Beukelman, D. R., Yorkston, K. M., & Reichle, J. (Eds.) Augmentative and Alternative Communication for adults with acquired neurologic disorders. Baltimore: Paul H. Brookes Publishing. 107-136.
- Schön, D. A. (1983). The reflective practitioner: How professionals think in action. New York: Basic books.